Organization of treatment and rehabilitation in Germany.
Complete medical support.
Complete medical support.
+49 176 17917001
All departments
The rotator cuff is a group of four muscles and tendons providing stability and mobility to the shoulder joint. Rotator cuff tears are among the most common causes of shoulder pain and weakness, especially in people over 40. With age, prevalence increases: after 60, partial or complete tears are found in 30–50% of people. Treatment in Germany includes arthroscopic repair, innovative MIBRAR® therapy for biological healing enhancement, and individualized rehabilitation.
The four cuff muscles "embrace" the humeral head, holding it in the glenoid socket. The supraspinatus initiates abduction (0–30°) and depresses the humeral head — it is damaged most often (>90% of tears). The infraspinatus provides external rotation. The teres minor assists with external rotation and depression. The subscapularis provides internal rotation. The supraspinatus tendon passes through a narrow space between the humeral head and acromion — this is where impingement syndrome develops, leading to degeneration and tearing.
Degenerative tears (85%) result from chronic tendinopathy plus impingement — the tendon gradually wears and tears with minimal loading. Traumatic tears (15%) result from falls on the arm, sudden jerks, or shoulder dislocations, typically in patients under 40. A "critical vascularity zone" exists in the supraspinatus tendon 1 cm from bone attachment with minimal blood supply — this is where degeneration begins. Risk factors include age >40, impingement syndrome, smoking, diabetes, dominant arm, and overhead work.
Partial tears damage part of the tendon thickness, with the articular side affected 3 times more often than the bursal side — they may heal with proper treatment. Full-thickness (transmural) tears represent through-and-through defects that do not heal spontaneously and progress. The Cofield classification grades them as small (<1 cm), medium (1–3 cm), large (3–5 cm), and massive (>5 cm). Massive irreparable tears involve tendon retraction plus fatty muscle degeneration where repair is technically impossible.
Shoulder pain along the anterolateral surface radiating to the deltoid area worsens with arm elevation. Night pain preventing sleep on the affected side is a hallmark symptom. Weakness makes it difficult to raise the arm overhead or hold objects at arm's length. A painful arc of 60–120° indicates impingement. Crepitus occurs with movement. Atrophy of the supraspinatus and/or infraspinatus muscles becomes visible in chronic tears. Pseudoparalysis — inability to actively raise the arm — indicates massive tears.
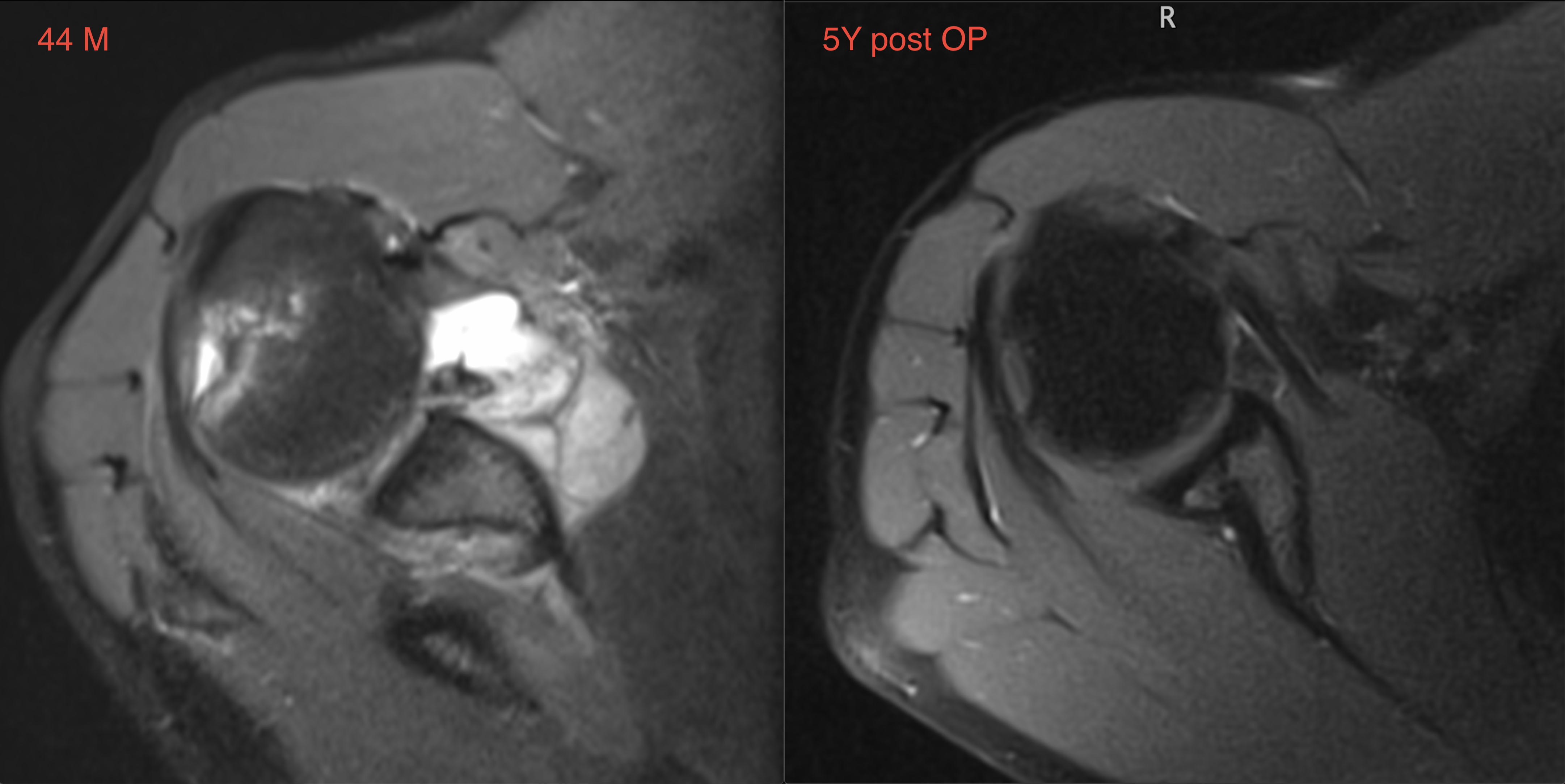
Clinical tests include Jobe (empty can — supraspinatus), Patte (external rotation — infraspinatus), Lift-off and Bear-hug (subscapularis), and drop arm (inability to hold the arm). Shoulder ultrasound is highly informative with 85–95% sensitivity for full tears. MRI is the gold standard for preoperative assessment, determining tear size, tendon retraction, fatty muscle degeneration (Goutallier classification — key to repair feasibility), and cartilage/labrum status. Radiography shows high-riding humeral head in massive tears, acromial osteophytes, and acromioclavicular arthrosis.
Indicated for partial tears, degenerative small tears in inactive elderly patients, and massive irreparable tears. Exercise therapy strengthens compensatory muscles (deltoid, infraspinatus) and stretches the posterior capsule. NSAIDs are used in courses during flares. Subacromial injections of corticosteroid reduce inflammation — limited to 2–3 injections as cortisone weakens tendons. Physiotherapy includes shockwave, ultrasound, and electrostimulation.
Rotator cuff tears are included in the indications for MIBRAR® technology. For partial tears, ARC transplantation directly into the damage zone stimulates tendon collagen regeneration — growth factors and mesenchymal stem cells trigger healing in the "critical vascularity zone" where blood supply is minimal. For biological augmentation of arthroscopic repair, enriching the refixation zone with ARC improves tendon-to-bone healing, reducing re-tear risk (up to 20–30% by global statistics). For tendinopathy without tear, degenerated tendon regeneration prevents progression to complete tear. For bursitis elimination, the powerful anti-inflammatory ARC effect works without cortisone.
ARC is delivered precisely under Sono Control Arm™ guidance (0.1 mm precision) into the tendon and subacromial space. Outpatient, without anesthesia. CGF method (Medifuge MF 200) + LIPOGEMS® ensure maximum regenerative factor concentration.
Indicated for full tears in active patients, traumatic tears, progressive weakness, and conservative treatment failure over 3–6 months. Modern technique in German clinics uses 3–4 punctures of 5 mm. The tendon is pulled to bone and fixed with anchor systems using single-row or double-row technique (suture bridge — the gold standard for medium and large tears). Simultaneous subacromial decompression removes acromial osteophytes preventing impingement recurrence. For massive irreparable tears: debridement, partial repair, tendon transfer (latissimus dorsi), balloon spacers (InSpace™), or reverse shoulder replacement (in elderly).
Phase 1 (0–6 weeks): immobilization in an abduction sling, passive movements, cryotherapy. Phase 2 (6–12 weeks): active-assisted movements, range of motion restoration. Phase 3 (3–6 months): rotator cuff and scapular stabilizer strengthening. Phase 4 (6–9 months): full activity and return to sports.
| Service | Price, € | Note |
|---|---|---|
| Diagnostics (MRI + ultrasound + exam) | 2,500–4,500 | 1 day |
| MIBRAR® therapy | on request | outpatient |
| Arthroscopic repair (small/medium) | 8,000–14,000 | 1–3 days inpatient |
| Arthroscopic repair (large/massive) | 12,000–18,000 | 2–4 days inpatient |
| Reverse shoulder replacement | 18,000–28,000 | 5–7 days inpatient |
All treatment prices in Germany.
Germany offers precise preoperative assessment with MRI, ultrasound, and Goutallier classification, MIBRAR® therapy for tendon regeneration and biological repair augmentation, double-row arthroscopic technique (suture bridge) for maximum contact area, solutions for massive irreparable tears (transfer, spacer, replacement), phased rehabilitation at specialized clinics, and multilingual assistance.
Rotator cuff tears progress over time — the earlier treatment begins, the better the outcome. Contact us for surgeon selection and a treatment program in Germany.








 +49 176 17917001
+49 176 17917001 
Or send us a message:



















