Organization of treatment and rehabilitation in Germany.
Complete medical support.
Complete medical support.
+49 176 17917001
All departments
Spondylolisthesis is a pathological displacement of one vertebra relative to the one below. The lumbar region (L4–L5, L5–S1) is most commonly affected. The condition may remain asymptomatic for years, but as it progresses it leads to chronic back pain, spinal canal stenosis, and neurological deficits. Treatment of spondylolisthesis in Germany includes precise diagnostics, modern minimally invasive surgery, and innovative MIBRAR® therapy for strengthening spinal tissues.
In spondylolisthesis, the vertebral body slides forward (anterolisthesis — 95% of cases) or backward (retrolisthesis) relative to the vertebra below. This disrupts the stability of the spinal segment and can lead to narrowing of the spinal canal and compression of neural structures. The most vulnerable levels are L5–S1 in the isthmic (spondylolytic) type, characteristic of young athletes, and L4–L5 in the degenerative type, characteristic of patients over 50.
Five types of spondylolisthesis are distinguished by cause (Wiltse–Newman classification):
| Type | Cause | Who is Affected | Level |
|---|---|---|---|
| I. Dysplastic | Congenital anomaly of the vertebral arch | Children, adolescents | L5–S1 |
| II. Isthmic | Defect in the pars interarticularis (spondylolysis) | Athletes, young adults | L5–S1 |
| III. Degenerative | Facet joint arthrosis, disc degeneration | Patients 50+ years | L4–L5 |
| IV. Traumatic | Fracture of the arch or articular processes | After injury | Any |
| V. Pathological | Bone tissue destruction (tumor, infection) | With osteomyelitis, tumors | Any |
The most common types are degenerative (in elderly) and isthmic (in young). In Germany, precise determination of the spondylolisthesis type is critically important for treatment selection.
The Meyerding classification is used to assess severity:
| Grade | Slippage | Approach |
|---|---|---|
| I | Up to 25% | Conservative treatment, exercise therapy, MIBRAR® |
| II | 25–50% | Conservative or surgical (if progressing) |
| III | 50–75% | Surgical treatment (stabilization) |
| IV | Over 75% | Surgical treatment (reduction + stabilization) |
| V (spondyloptosis) | Complete slip-off | Emergency surgery |
The clinical picture depends on the degree of slippage and presence of neural compression. Pain syndrome manifests as lower back pain worsening with extension, prolonged standing and walking, improving in seated position and with forward flexion. Patients often describe a feeling of "instability" — the spine feels "loose" or "shifting." Muscle spasms in the lumbar area are common.
When neural compression develops, radicular pain radiating to the buttock and leg, numbness and tingling in the legs, foot weakness, neurogenic claudication (with concomitant canal stenosis), and pelvic organ dysfunction in severe spondyloptosis may occur.
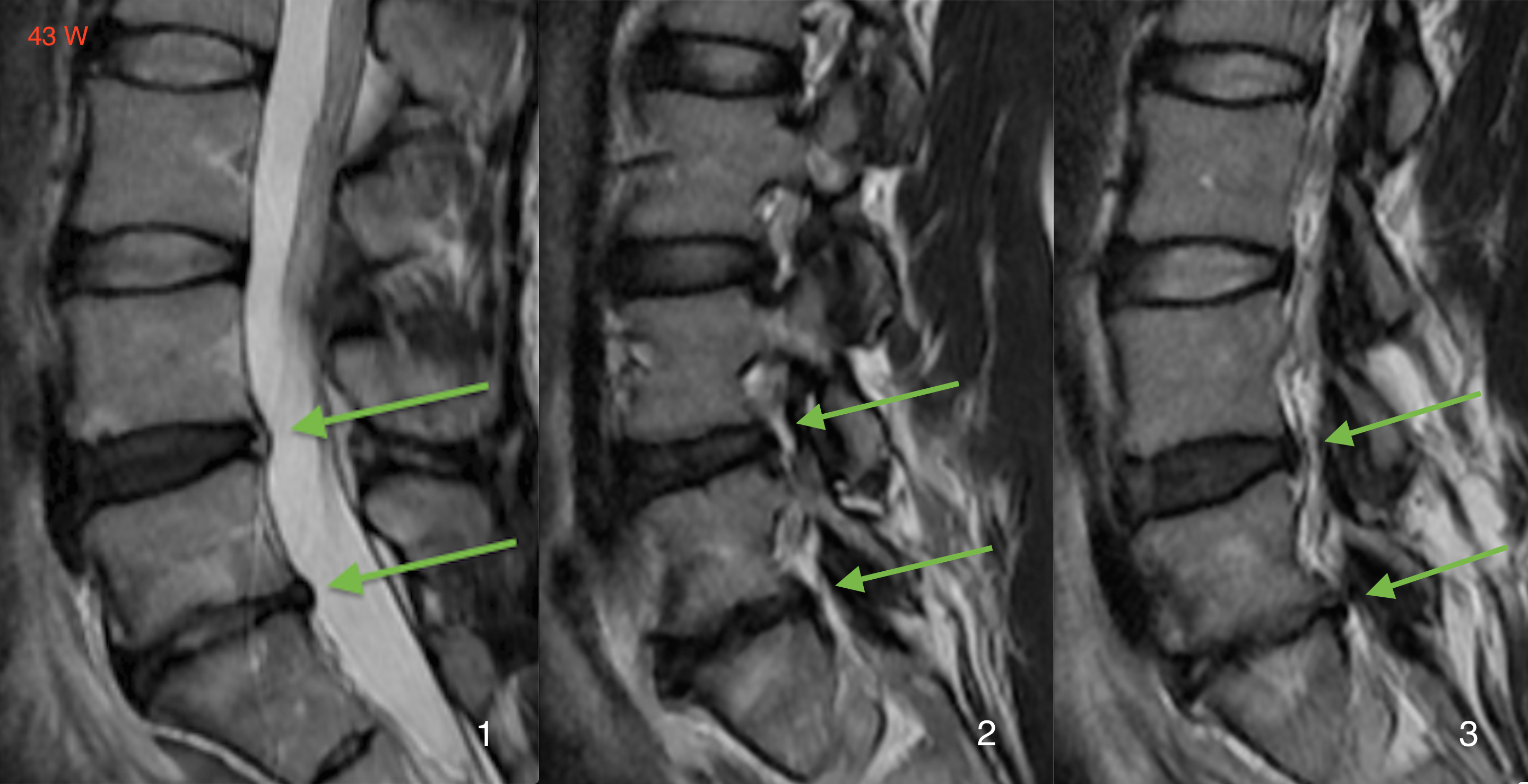
Functional radiography — flexion and extension views — is the key investigation, allowing assessment of slippage degree and identification of unstable (mobile) forms. Spinal MRI evaluates disc condition, neural structures, spinal cord, and facet joints. CT provides detailed bone structure visualization and identification of spondylolysis (arch defect). SPECT/CT or PET/CT is used when active spondylolysis is suspected in young athletes. EMG is performed for neurological symptoms to assess nerve root damage. Diagnostic facet blocks confirm the pain source. Comprehensive examination in Germany takes 1–2 days, after which a neurosurgeon-orthopedist team determines the individual treatment strategy.
For grade I–II without progression or neurological deficit, non-surgical methods are initiated. Exercise therapy focusing on strengthening spinal stabilizer muscles (multifidus, transversus abdominis) is the most fundamental and important treatment component. Drug therapy with NSAIDs and muscle relaxants is used during flares. Physiotherapy includes electrostimulation, ultrasound, and thermal procedures. Semi-rigid bracing provides support during instability. Epidural injections are used for pain flares with radiculopathy. Facet blocks and radiofrequency ablation address concomitant facet syndrome.
Spondylolisthesis is included in the indications for innovative MIBRAR® technology. The method is particularly effective for degenerative spondylolisthesis, when the cause of slippage is disc and facet joint destruction.
MIBRAR® for spondylolisthesis achieves degenerated disc regeneration restoring height and shock-absorbing function, facet joint cartilage regeneration for segment stabilization, ligamentous apparatus strengthening through growth factor-stimulated collagen synthesis, and slippage correction — during ARC implantation into the disc, increased intradiscal pressure pulls the displaced vertebra back into position through longitudinal ligament tension (data from Prof. Babayan's book: complete correction of ventral and retrolisthesis).
The procedure is performed on an outpatient basis, without anesthesia or incisions. A spinal probe (0.8 mm) is introduced into the disc under Sono Control Arm™ guidance (0.1 mm precision) or X-ray navigation with Cyber-Navi-Hand™. Only the patient's own tissues are used — no prostheses, screws, or cortisone.
Surgical indications include progressive slippage (increasing grade on follow-up images), neurological deficit (weakness, sensory disturbance, pelvic organ dysfunction), persistent pain syndrome not responding to conservative treatment for 3–6 months, grade III–IV slippage, and pronounced spinal canal stenosis.
Surgical methods in German clinics include decompression with transpedicular fixation (removing causes of nerve compression + stabilization with screws and rods — the gold standard), interbody fusion (TLIF/PLIF/ALIF — cage placement in the removed disc space + transpedicular fixation for 360° stabilization), minimally invasive fusion (MIS-TLIF — the same operation through small incisions using tubular retractors and navigation, with less blood loss and faster recovery), and reduction for severe spondylolisthesis (partial or complete repositioning of the displaced vertebra before fixation).
Success rate of surgical spondylolisthesis treatment in German clinics is 85–95%. The patient stands on the day of surgery.
The recovery program includes mobilization on the day of surgery, brace wearing for 6–12 weeks, exercise therapy starting with isometric exercises from the first days and muscle strengthening from week 6, aquatic gymnastics from weeks 4–6, full return to active life within 3–6 months, and follow-up radiography at 3, 6 and 12 months.
| Service | Price, € | Note |
|---|---|---|
| Diagnostics (MRI + functional X-ray + consultation) | 3,500–6,000 | 1–2 days |
| Conservative course | 5,000–8,000 | 7–14 days |
| MIBRAR® therapy | on request | outpatient |
| Decompression + stabilization (1 segment) | 20,000–30,000 | 5–7 days inpatient |
| TLIF fusion (1 segment) | 22,000–35,000 | 5–10 days inpatient |
All treatment prices in Germany.
Germany offers precise classification of slippage type and grade, MIBRAR® therapy for disc and facet joint regeneration in the degenerative type, minimally invasive navigated surgery for accuracy and safety, years of German neurosurgical experience in stabilizing operations, complete rehabilitation at world-class clinics, and multilingual assistance at every stage.
Spondylolisthesis requires qualified monitoring and treatment. Contact us — we will develop the optimal strategy at the best clinics in Germany.








 +49 176 17917001
+49 176 17917001 
Or send us a message:



















