Organization of treatment and rehabilitation in Germany.
Complete medical support.
Complete medical support.
+49 176 17917001
All departments
Cruciate ligament tear is one of the most serious injuries in orthopedics. The anterior cruciate ligament (ACL) tears 10 times more frequently than the posterior (PCL). Over 200,000 ACL reconstructions are performed annually in Europe. Without treatment, an ACL tear leads to progressive knee instability, recurrent subluxations, meniscal damage, and rapid development of gonarthrosis. Cruciate ligament treatment in Germany represents world-class arthroscopic surgery enhanced by innovative MIBRAR® therapy for improved graft integration.
The cruciate ligaments are located inside the knee joint and cross each other (hence the name). The anterior cruciate ligament (ACL) prevents anterior tibial translation and internal rotation, consisting of two bundles: anteromedial (taut in flexion) and posterolateral (taut in extension), measuring 30–35 mm in length and 10–12 mm in thickness. The posterior cruciate ligament (PCL) prevents posterior tibial translation and is 1.5–2 times stronger than the ACL. The ACL is the key knee stabilizer — its tear fundamentally alters joint biomechanics, increasing stress on menisci and cartilage.
ACL tears (90% of cases) most commonly occur through a non-contact mechanism (70%) — sudden deceleration plus pivoting with a planted foot, typical in football, alpine skiing, and basketball. Contact injuries result from a blow to the outer knee with a bent leg (valgus stress). Hyperextension (knee overextension) is another mechanism. PCL tears (10%) typically result from a blow to the anterior tibia with a flexed knee (dashboard injury in motor vehicle accidents) or falling onto a flexed knee. Combined injuries — ACL plus medial collateral ligament plus medial meniscus — constitute the "unhappy triad" (O'Donoghue). In 50–70% of ACL tears, concomitant meniscal damage occurs.
In the acute period, a characteristic pop or crack at the moment of injury is the hallmark ACL sign. Rapid swelling (hemarthrosis) develops within 2–6 hours as the knee "balloons." Intense pain prevents continuation of sports activity. A sense of instability — "the knee came apart" or "gave way" — is described. Limited motion with inability to fully extend the knee completes the picture.
Chronic instability without treatment manifests as recurrent "giving way" episodes (knee buckling during turning, descending stairs), recurrent synovitis with swelling after activity, secondary meniscal and cartilage damage, and progressive arthrosis.
The clinical examination employs the Lachman test (the most sensitive at 85–95%), anterior drawer test, and pivot-shift test (rotational subluxation). For PCL: posterior drawer test and sag-sign (tibial sagging). Knee MRI is the gold standard with 90–95% accuracy for ACL tears, evaluating tear type (complete/partial), concomitant injuries (menisci, cartilage, collateral ligaments, bone bruise). Radiography excludes fractures and identifies Segond fracture (lateral tibial plateau avulsion — pathognomonic for ACL tear). Arthrometry (KT-1000) provides instrumental measurement of anteroposterior tibial translation, with >3 mm difference from the healthy side confirming the diagnosis.
ACL reconstruction is indicated for young active patients (athletes, physically active workers), pronounced instability (positive pivot-shift), combined injuries (ACL plus meniscus), recurrent subluxations, and desire to return to pivoting sports (football, skiing, basketball). Conservative treatment (without surgery) is possible for inactive older patients with compensated instability, provided powerful muscular stabilization (exercise therapy) is maintained.
Modern ACL reconstruction is performed arthroscopically through 2–3 punctures of 5 mm. The torn ligament cannot be sutured (it will not heal!) and is replaced with a graft. Graft options include BTB (bone-tendon-bone) using the middle third of the patellar tendon with bone blocks providing strong bone-to-bone fixation, hamstring (ST/G) using semitendinosus and gracilis tendons (most popular, minimal donor site pain), quadriceps tendon (thick graft gaining popularity), and allograft (donor tendon — no donor site morbidity but slower integration).
German surgeons select the graft individually based on age, activity, knee anatomy, and patient preference. The anatomic technique recreates the natural ligament position using precise bone tunnel placement with 3D navigation and arthroscopic control for maximum accuracy.
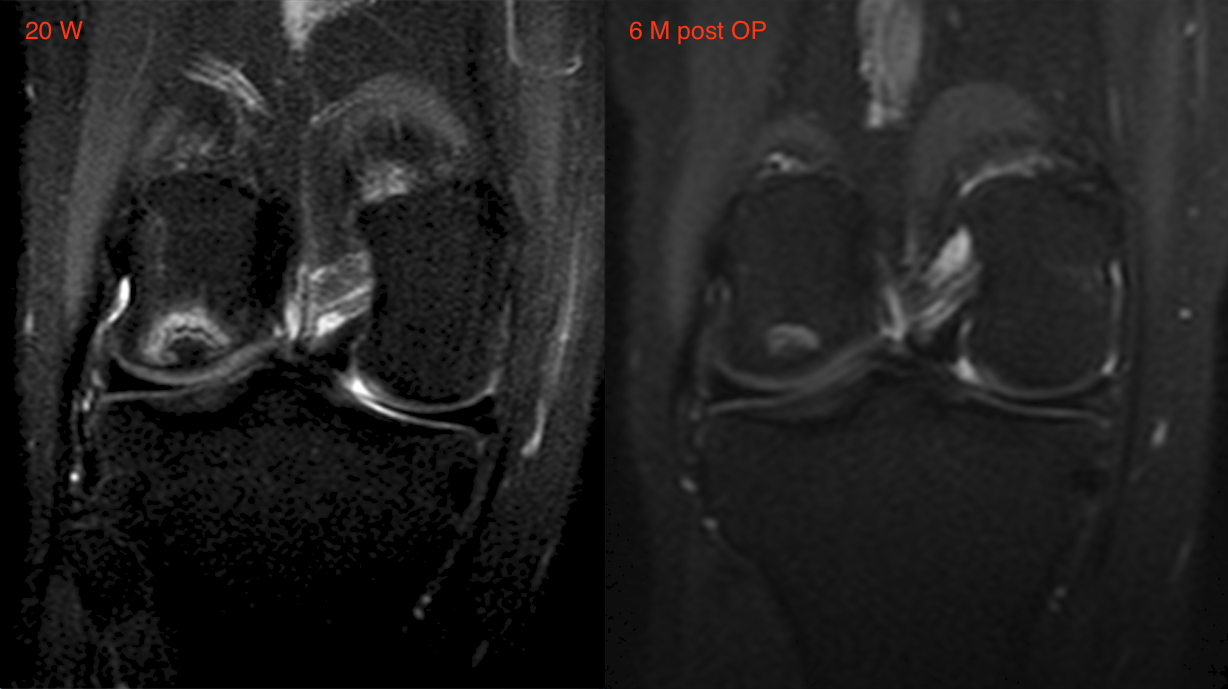
Cruciate ligament tear (Kreuzbandriss) is included in the indications for MIBRAR® technology. For partial ACL tears, intraligamentous ARC transplantation stimulates fiber regeneration without the need for reconstruction — particularly effective in young patients with good vascularity. For biological augmentation of reconstruction, intraoperative ARC transplantation into the graft zone and bone tunnels accelerates integration and remodeling, with faster bone incorporation. For concomitant damage, simultaneous meniscal and cartilage treatment with ARC provides comprehensive joint restoration. For arthrosis prevention, joint cartilage regeneration slows post-traumatic arthrosis development.
ARC contains growth factors (CGF method, Medifuge MF 200 centrifuge), mesenchymal stem cells (LIPOGEMS®), and anti-inflammatory factors. The procedure supplements arthroscopy or is performed independently for partial tears under Sono Control Arm™ guidance without anesthesia.
| Phase | Timeline | Goals and Activities |
|---|---|---|
| 1 | 0–2 wks | Swelling reduction, full extension, quadriceps activation. Crutch walking, partial weight bearing |
| 2 | 2–6 wks | Full weight bearing, flexion to 120°, proprioception, stationary cycling |
| 3 | 6–12 wks | Muscle strengthening, straight-line jogging (from 10–12 wks), swimming |
| 4 | 3–6 mo | Functional training, jumping, direction changes |
| 5 | 6–9 mo | Return to sports (upon passing functional tests) |
| Service | Price, € | Note |
|---|---|---|
| Diagnostics (MRI + examination + arthrometry) | 2,500–4,500 | 1 day |
| MIBRAR® therapy (partial tear) | on request | outpatient |
| Arthroscopic ACL reconstruction | 10,000–16,000 | 2–3 days inpatient |
| ACL reconstruction + meniscus repair + MIBRAR® | 14,000–20,000 | 2–3 days inpatient |
| Revision ACL reconstruction | 15,000–22,000 | 3–5 days inpatient |
All treatment prices in Germany.
Germany offers anatomic arthroscopic reconstruction with 3D navigation, MIBRAR® therapy accelerating graft integration and cartilage regeneration, individual graft selection, comprehensive treatment of concomitant meniscal, cartilage, and collateral ligament injuries, phased rehabilitation with functional testing, surgeons with thousands of annual ACL reconstructions at specialized clinics, and multilingual assistance.
A cruciate ligament tear is not a career-ending injury. Contact us — we will find a world-class surgeon for your case.








 +49 176 17917001
+49 176 17917001 
Or send us a message:



















