Organization of treatment and rehabilitation in Germany.
Complete medical support.
Complete medical support.
+49 176 17917001
All departments
Meniscus tear is one of the most common knee injuries. Over 300,000 knee arthroscopies are performed annually in Germany, with a significant proportion related to meniscal injuries. German orthopedics adheres to the principle of maximum meniscus preservation: repair over removal, regeneration over resection. Innovative MIBRAR® therapy opens new possibilities for healing damaged meniscus without surgery or as a complement to it.
Each knee joint contains two menisci — crescent-shaped cartilage pads between the femur and tibia. The medial (inner) meniscus is less mobile and is damaged 3–4 times more often. The lateral (outer) meniscus is more mobile and better "escapes" injury. Menisci serve critical functions: they absorb up to 70% of impact loading during walking and running, stabilize the joint by deepening the articular surface and preventing subluxation, distribute load by increasing the contact area by 60%, lubricate the joint by distributing synovial fluid, and provide proprioception through nerve endings participating in movement coordination.
Meniscus removal increases contact pressure on cartilage 2–3 fold, inevitably leading to knee arthrosis. This is precisely why German surgeons strive to preserve the meniscus at all costs.
Traumatic tears result from rotational injury (knee twisting with a planted foot) — the most common mechanism in football, skiing, basketball, and tennis. Deep squatting or rising from a deep squat also causes tears. Combined injuries involving meniscus plus cruciate ligament (O'Donoghue's triad) are particularly serious.
Degenerative tears occur in patients over 40 as the meniscus loses elasticity with age, and may happen during minimal loading (climbing stairs, squatting). They often coexist with knee arthrosis. Risk factors include excess weight and varus/valgus leg deformity.
Classification by type and location is critical for treatment selection:
| Tear Type | Description | Treatment Approach |
|---|---|---|
| Longitudinal (vertical) | Tear along meniscal fibers | Meniscus repair (best healing prognosis) |
| Bucket-handle | Large longitudinal tear with fragment displacement | Emergency repair (joint locking!) |
| Radial | Tear perpendicular to fiber direction | Repair or partial meniscectomy |
| Horizontal | Meniscus delamination into two layers | Repair or partial meniscectomy |
| Flap | Tissue flap detachment | Partial meniscectomy of unstable flap |
| Complex | Combination of several types | Individual approach |
Blood supply zones are the key factor determining healing prognosis. The red zone (peripheral third) has good blood supply with 85–90% repair success. The red-white zone (middle third) has moderate blood supply with 60–70% repair success — where MIBRAR® significantly improves healing chances. The white zone (inner third) has minimal blood supply with difficult healing, suitable for partial resection or MIBRAR® stimulation.
Acute traumatic tears present with sudden knee pain at the moment of injury, a characteristic click or pop, rapidly developing swelling (within hours), limited motion (inability to fully extend the knee), and joint locking — the "stuck knee" of bucket-handle tears.
Chronic or degenerative tears manifest as intermittent pain along the inner or outer knee joint line, pain descending stairs (a characteristic symptom!), clicking and feeling of "giving way," episodic locking, and joint swelling after activity.
The clinical examination employs specific tests: McMurray (rotation + extension), Apley (compression + rotation), and Thessaly (rotation on a weight-bearing leg at 20° flexion) with 70–90% combined sensitivity. Knee MRI is the gold standard with 90–95% diagnostic accuracy for meniscal tears, determining type, location, blood supply zone, and cartilage and ligament condition. Radiography excludes fractures, evaluates leg axis, and identifies arthrosis signs. Knee ultrasound assesses effusion, meniscal cleft, and meniscal cysts. Diagnostic arthroscopy allows direct meniscal inspection and immediate treatment when needed. Examination in German clinics takes 1 day, after which the surgeon-orthopedist determines the individual approach.
Non-surgical treatment is indicated for small stable tears (less than 5 mm) in the red zone, degenerative tears without mechanical symptoms (locking), and elderly patients with concomitant arthrosis. The program includes immobilization with an orthosis or splint for 2–4 weeks with gradual range of motion increase, cryotherapy for acute swelling, NSAIDs for pain and inflammation, exercise therapy for quadriceps strengthening and proprioception restoration, and physiotherapy including electromyostimulation, ultrasound, and magnetotherapy.
Knee arthroscopy is a minimally invasive operation through two 5 mm punctures. German surgeons use HD cameras providing multiple magnification.
Meniscus repair (meniscopexy) is the preferred method for maximum tissue preservation. It is indicated for tears in red and red-white zones, fresh tears (up to 6 weeks), and longitudinal tears. Techniques include all-inside (anchor systems), inside-out, and outside-in approaches. Healing success reaches 80–95% in the red zone. Rehabilitation takes longer (6–12 weeks of weight-bearing restriction) but the joint remains fully functional.
Partial meniscectomy removes only the damaged fragment and is indicated when repair is impossible — in white zone tears, degenerative complex tears, and old injuries with tissue degeneration. German surgeons remove the minimum possible tissue volume, striving to preserve the meniscal rim for joint stability. For complete meniscal loss in young patients, meniscal transplantation using a donor meniscus is performed at selected specialized German centers.
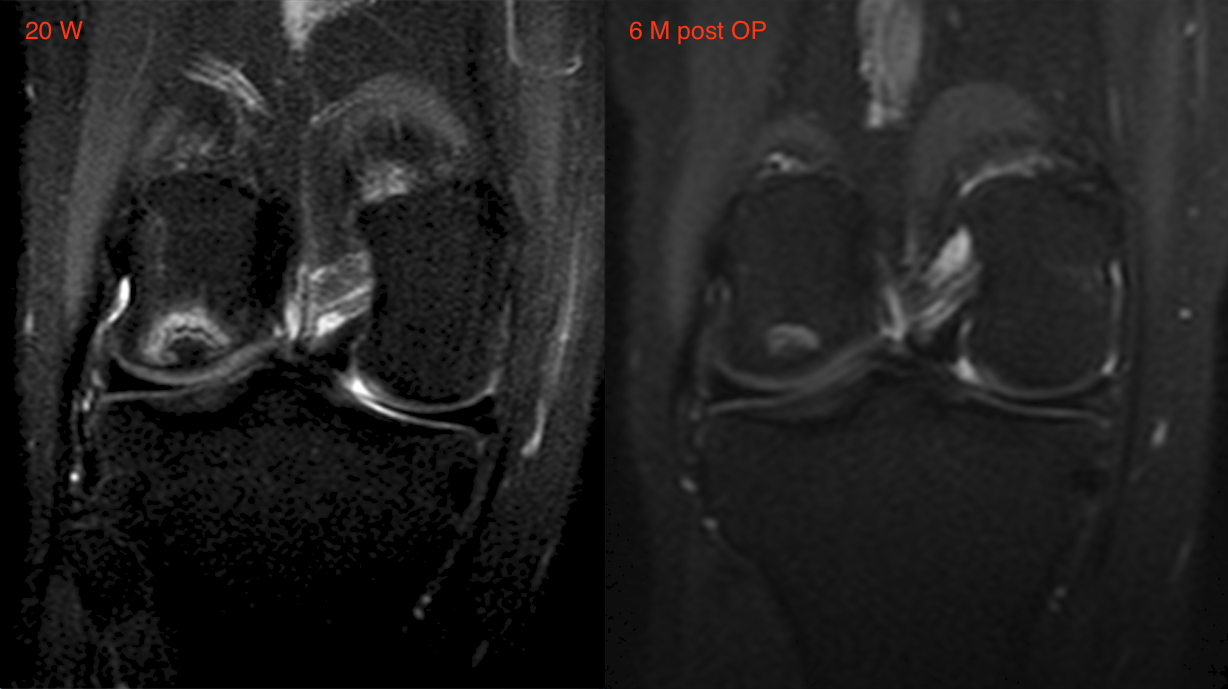
Meniscus tear is included in the indications for innovative MIBRAR® technology, significantly expanding treatment possibilities. For conservative treatment, autologous regenerative concentrate (ARC) injection into the tear zone stimulates healing even in poorly vascularized zones. As a complement to meniscus repair, enriching the repair zone with growth factors and stem cells raises healing success from 60–70% to 85–90% in the red-white zone. For concomitant arthrosis, MIBRAR® simultaneously regenerates joint cartilage. For meniscal cysts, the method eliminates the cyst-forming cause.
The MIBRAR® procedure is performed under ultrasound guidance (Sono Control Arm™, 0.1 mm precision), on an outpatient basis without anesthesia. ARC contains growth factors, mesenchymal stem cells, and anti-inflammatory factors from the patient's own blood and adipose tissue — with no risk of allergic reactions.
The recovery program depends on the intervention performed:
| Operation | Weight Bearing | Sports | Full Recovery |
|---|---|---|---|
| Partial meniscectomy | Immediate, full | 3–6 weeks | 4–8 weeks |
| Meniscus repair | Partial 6 wks, full from 8 wks | 4–6 months | 3–6 months |
Rehabilitation stages progress from cryotherapy and isometric exercises with crutch walking (weeks 1–2), through increased range of motion, thigh strengthening, and balance exercises (weeks 3–6), to full weight bearing, stationary cycling, swimming, and proprioceptive training (weeks 6–12), and finally functional training and return to sports after meniscus repair (months 3–6).
| Service | Price, € | Note |
|---|---|---|
| Diagnostics (MRI + examination) | 2,500–4,000 | 1 day |
| Arthroscopic meniscectomy | 5,000–8,000 | 1–2 days inpatient |
| Arthroscopic meniscus repair | 7,000–12,000 | 1–3 days inpatient |
| MIBRAR® therapy | on request | outpatient |
| Meniscus transplantation | 15,000–22,000 | 3–5 days inpatient |
All treatment prices in Germany.
Germany upholds the "meniscus preservation first" principle — repair over removal. MIBRAR® therapy provides biological healing stimulation with growth factors. HD arthroscopy through minimal 5 mm incisions is performed by surgeons with thousands of annual arthroscopies at specialized clinics, with rapid rehabilitation and multilingual assistance at every stage.
Don't delay treatment — a fresh meniscus tear has a significantly better prognosis. Contact us for doctor and clinic selection in Germany.








 +49 176 17917001
+49 176 17917001 
Or send us a message:



















