Organization of treatment and rehabilitation in Germany.
Complete medical support.
Complete medical support.
+49 176 17917001
All departments
Disc degeneration (degenerative disc disease — DDD) is a progressive process of cartilage tissue destruction in which discs lose moisture, height and shock-absorbing capacity. This is the primary cause of osteochondrosis, disc herniations and chronic back pain. Disc degeneration treatment in Germany opens unique possibilities — from comprehensive diagnostics to innovative MIBRAR® therapy capable of restoring the structure of a damaged disc.
The intervertebral disc consists of two main components. The nucleus pulposus — a gel-like center, 80% water — is responsible for shock absorption and load distribution. The annulus fibrosus — a strong outer shell of collagen fibers — holds the nucleus in place. During degeneration, the nucleus dehydrates, the annulus develops microcracks, and disc height decreases. This disrupts the biomechanics of the entire spinal segment: facet joints become overloaded, instability develops, and protrusions and herniations form.
It is crucial to understand that the disc has no blood vessels of its own. Nutrition occurs through diffusion from surrounding tissues. This is precisely why the disc recovers extremely poorly on its own, and special methods are required for regeneration.
Disc degeneration is a multifactorial process. Age is the leading factor — starting from age 20–25, disc water content gradually decreases, and by 60 nearly everyone shows degeneration signs on MRI. Genetics plays a significant role, with studies showing that up to 70% of degeneration risk is determined by genes. Smoking narrows blood vessels and impairs nutrient diffusion into disc tissue. Excess weight increases axial loading on the spine, especially the lumbar region. Heavy physical labor involving vibration, weight lifting and prolonged spinal loading accelerates degeneration. Conversely, a sedentary lifestyle disrupts diffuse disc nutrition. Injuries such as vertebral fractures and compressive injuries accelerate degeneration. Metabolic disorders including diabetes and calcium metabolism disturbances also contribute.
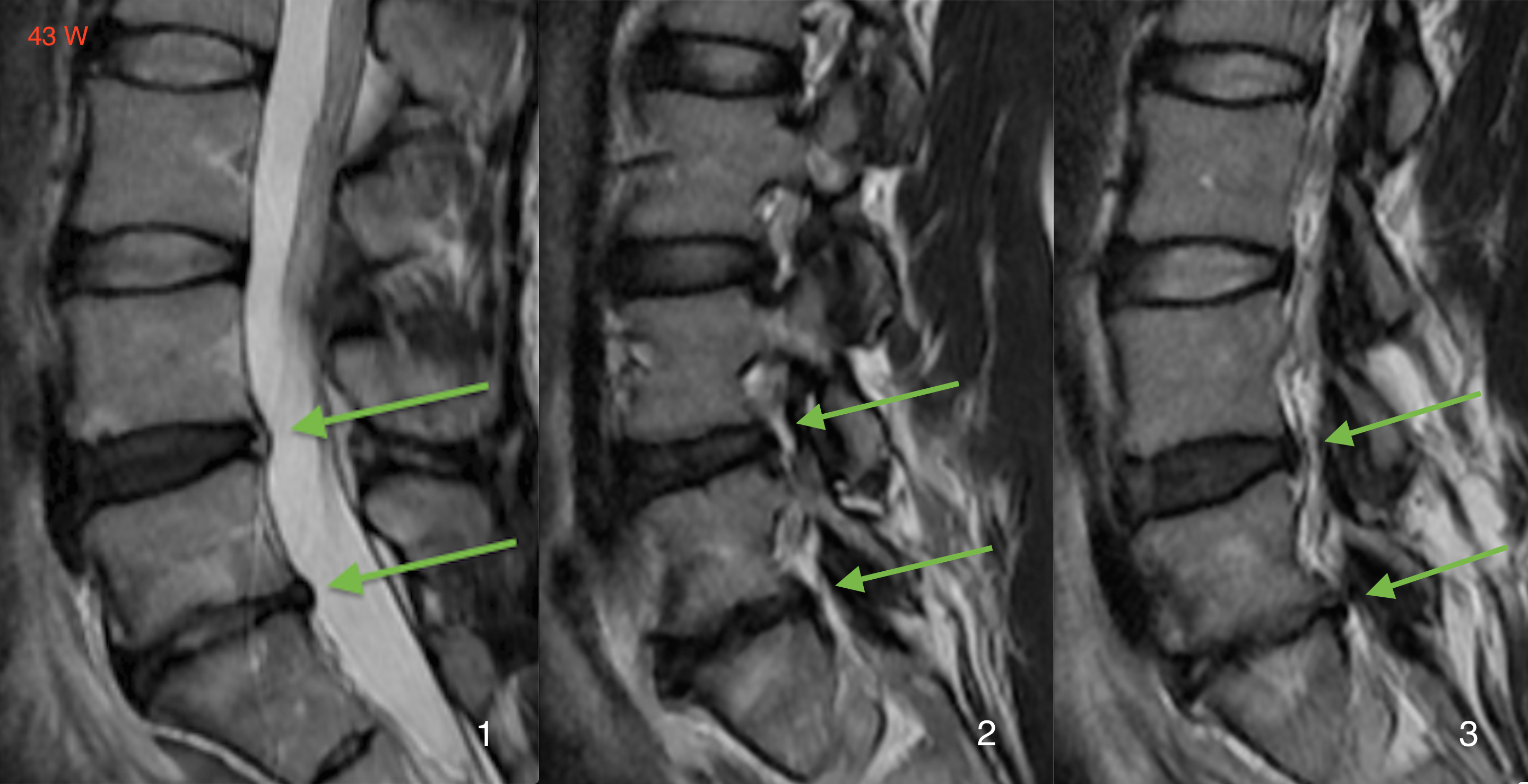
The Pfirrmann classification (used by German physicians for MRI assessment) distinguishes five grades:
| Grade | Disc Structure | MRI Signal | Disc Height | Clinical Picture |
|---|---|---|---|---|
| I | Homogeneous, bright | Hyperintense | Normal | Asymptomatic |
| II | Inhomogeneous, with horizontal band | Hyperintense | Normal | Mild discomfort |
| III | Inhomogeneous, gray | Intermediate | Slightly decreased | Pain during loading |
| IV | Inhomogeneous, dark | Hypointense | Decreased | Chronic pain |
| V | Disc collapse | Hypointense | Collapsed | Severe pain syndrome |
At stages I–III, regenerative methods including MIBRAR® are most effective. At stages IV–V, surgical intervention may be required.
Clinical manifestations of disc degeneration depend on the location and degree of involvement. Discogenic pain is typically deep and aching, worsening with prolonged sitting, bending and turning, and characteristically improving with walking and lying down. Morning stiffness is a typical symptom — after overnight rest the disc absorbs moisture, increases in volume and presses on surrounding tissues. Pain may radiate to the buttock and thigh with lumbar involvement, or to the shoulder and arm with cervical involvement. Muscle spasms represent reflexive tension of paravertebral muscles. Neurological symptoms including numbness and limb weakness develop with nerve root compression.
The insidious nature of the disease is that symptoms may be minimal in the early stages while the pathological process is already actively progressing. Early diagnosis is the key to successful treatment.
German clinics employ comprehensive diagnostics. Spinal MRI is the gold standard, assessing the degree of dehydration, disc heights, presence of herniations and protrusions, and Pfirrmann classification. Functional radiography with flexion/extension views evaluates instability. CT provides detailed bone structure visualization including osteophytes. Discography is a provocative test confirming discogenic pain by injecting contrast into the suspected disc. EMG/ENMG electrodiagnostics are used when neurological symptoms are present. Laboratory tests exclude spondylodiscitis and rheumatic diseases.
At stages I–III, non-surgical methods form the basis of treatment. Drug therapy includes NSAIDs for pain and inflammation relief, muscle relaxants for spasm relief, and chondroprotectors such as glucosamine and chondroitin sulfate. Epidural injections are used for pronounced pain syndrome. Physiotherapy encompasses therapeutic exercise for strengthening deep spinal stabilizers, manual therapy for segment mobilization and functional block elimination, traction therapy for disc decompression through spinal traction, shockwave therapy for regeneration stimulation, and aquatic gymnastics for simultaneous spine unloading and muscle training.
Disc degeneration is one of the key indications for the innovative MIBRAR® technology. Unlike all traditional methods that merely slow destruction, MIBRAR® can trigger the reverse process — restoration of disc structure.
The procedure works as follows: autologous regenerative concentrate (ARC) containing mesenchymal stem cells, growth factors and anti-inflammatory factors is obtained from the patient's blood and adipose tissue. Under ultrasound guidance (Sono Control Arm™, 0.1 mm precision), targeted microperforations are performed in the affected disc area. The ARC is then transplanted directly into the disc tissue through a puncture — without any incision.
Why MIBRAR® is more effective than standard PRP therapy: the certified Medifuge MF 200 centrifuge ensures maximum growth factor concentration; the concentrate contains not only platelet factors but also mesenchymal stem cells from adipose tissue; targeted delivery into the affected zone is performed under ultrasound guidance; Prof. Babayan's method has been applied in over 11,000 cases without significant side effects.
The result: on follow-up MRI at 8–16 weeks, increased disc height and restored hydration are observed. This is an objective, measurable outcome with no analogues in world practice.
For severe degeneration (stages IV–V) with pronounced pain syndrome and failure of conservative therapy, German surgeons employ disc replacement (replacing the destroyed disc with an artificial one, preserving segment mobility — particularly effective for cervical and lumbar regions), interbody fusion (TLIF/ALIF — disc removal and vertebral fixation with a cage, indicated for pronounced instability), microdiscectomy (when herniation has formed with neural structure compression), and nucleoplasty (minimally invasive disc volume reduction for protrusions).
The recovery program for disc degeneration includes therapeutic exercise for core stability training, manual therapy and massage, aquatic gymnastics including swimming and aqua aerobics, deep muscle electromyostimulation, ergonomic training covering proper posture and workstation organization, and weight reduction when necessary. Recovery time is 4–8 weeks after conservative treatment or MIBRAR®, and 8–12 weeks after surgery.
| Service | Price, € | Note |
|---|---|---|
| Diagnostics (MRI + consultation) | 3,000–5,000 | 1–2 days |
| Conservative course | 5,000–9,000 | 7–14 days |
| MIBRAR® therapy | on request | outpatient |
| Disc replacement | 20,000–35,000 | 5–7 days inpatient |
| Spinal fusion | 18,000–28,000 | 5–10 days inpatient |
All treatment prices in Germany.
Germany offers accurate diagnostics with international standard classification (Pfirrmann), exclusive MIBRAR® therapy — the world's only disc regeneration method, a multidisciplinary approach with neurosurgeons, orthopedists, neurologists and physiotherapists, minimally invasive surgery with rapid recovery when operation is needed, a full rehabilitation cycle at world-class clinics, and personal assistance throughout the treatment process.
Disc degeneration is not a death sentence. Modern technologies allow not only halting destruction but also triggering restoration. Contact us — we will develop an optimal treatment plan for you.








 +49 176 17917001
+49 176 17917001 
Or send us a message:



















