Organization of treatment and rehabilitation in Germany.
Complete medical support.
Complete medical support.
+49 176 17917001
All departments
Osteochondrosis is a chronic degenerative-dystrophic disease of the spine affecting intervertebral discs, vertebral bodies, the ligamentous apparatus and surrounding muscles. According to statistics, up to 80% of the population experiences back pain associated with osteochondrosis at least once in their lifetime. The disease significantly reduces quality of life and can lead to serious complications — disc herniations, spinal canal stenosis, nerve root compression. Osteochondrosis treatment in Germany enables halting destruction and triggering tissue regeneration thanks to cutting-edge technologies and innovative MIBRAR® therapy.
The intervertebral disc is a complex structure consisting of the nucleus pulposus (a gel-like center) and the annulus fibrosus (a dense outer shell). Discs act as shock absorbers, providing flexibility and mobility to the spine. In osteochondrosis, the disc loses moisture, becomes less elastic and decreases in height. This triggers a cascade of pathological changes: disruption of spinal segment biomechanics, overloading of facet joints, formation of protrusions and herniations, growth of bone spurs (osteophytes), and compression of neural structures and blood vessels.
The disease can affect any part of the spine: cervical (the most mobile), thoracic (the least common), and lumbar (bearing the maximum load). Multisegmental osteochondrosis with simultaneous involvement of several regions is not uncommon.
Osteochondrosis is a multifactorial disease. The main causes and provoking factors include genetic predisposition (hereditary weakness of connective tissue, structural features of the spine), physical inactivity (sedentary lifestyle, computer work — the main cause in young adults, as lack of movement impairs disc nutrition), excessive loading (heavy physical labor, professional sports, weight lifting), excess weight (each extra kilogram increases the load on the lumbar spine), spinal injuries (vertebral fractures, bruises, microtrauma during sports), postural disorders (scoliosis, kyphosis, lordosis creating uneven disc loading), age-related changes (after age 30, degenerative processes in discs accelerate), smoking (nicotine impairs microcirculation and cartilage nutrition), and metabolic disorders (diabetes, hypothyroidism, gout).
Osteochondrosis develops gradually. Doctors distinguish four stages of progression:
| Stage | Disc Changes | Symptoms | Prognosis |
|---|---|---|---|
| I | Dehydration of the nucleus pulposus, initial microcracks in the annulus | Mild discomfort, episodic pain | Full recovery with proper treatment |
| II | Decreased disc height, segment instability, protrusions | Persistent pain, muscle spasms, limited mobility | Conservative treatment is effective |
| III | Annulus rupture, disc herniations, nerve compression | Severe radiating pain, numbness, limb weakness | Comprehensive therapy required |
| IV | Osteophytes, ankylosis, disc fibrosis | Chronic pain syndrome, severe movement restriction | Surgical intervention may be needed |
The earlier osteochondrosis is detected, the higher the chances of full recovery. At stages I–II, it is possible to avoid surgery using innovative regenerative methods.
The clinical picture depends on the location and stage of the disease.
Pain in the neck radiating to the shoulder, arm and fingers is the most common symptom. Patients frequently report headaches, dizziness and tinnitus caused by compression of the vertebral arteries. Visual disturbances (floaters), numbness and tingling in the fingers, and stiffness when turning the head are also characteristic.
Intercostal neuralgia — pain mimicking cardiac pain — is the hallmark of thoracic involvement. Pain between the shoulder blades that worsens with deep breathing and discomfort during prolonged sitting are typical complaints.
Lumbago — acute shooting pain in the lower back — is often the first manifestation. Sciatica (pain radiating along the back of the leg), numbness and weakness in the legs, pelvic organ dysfunction in severe cases, and limited bending and trunk rotation complete the clinical picture.
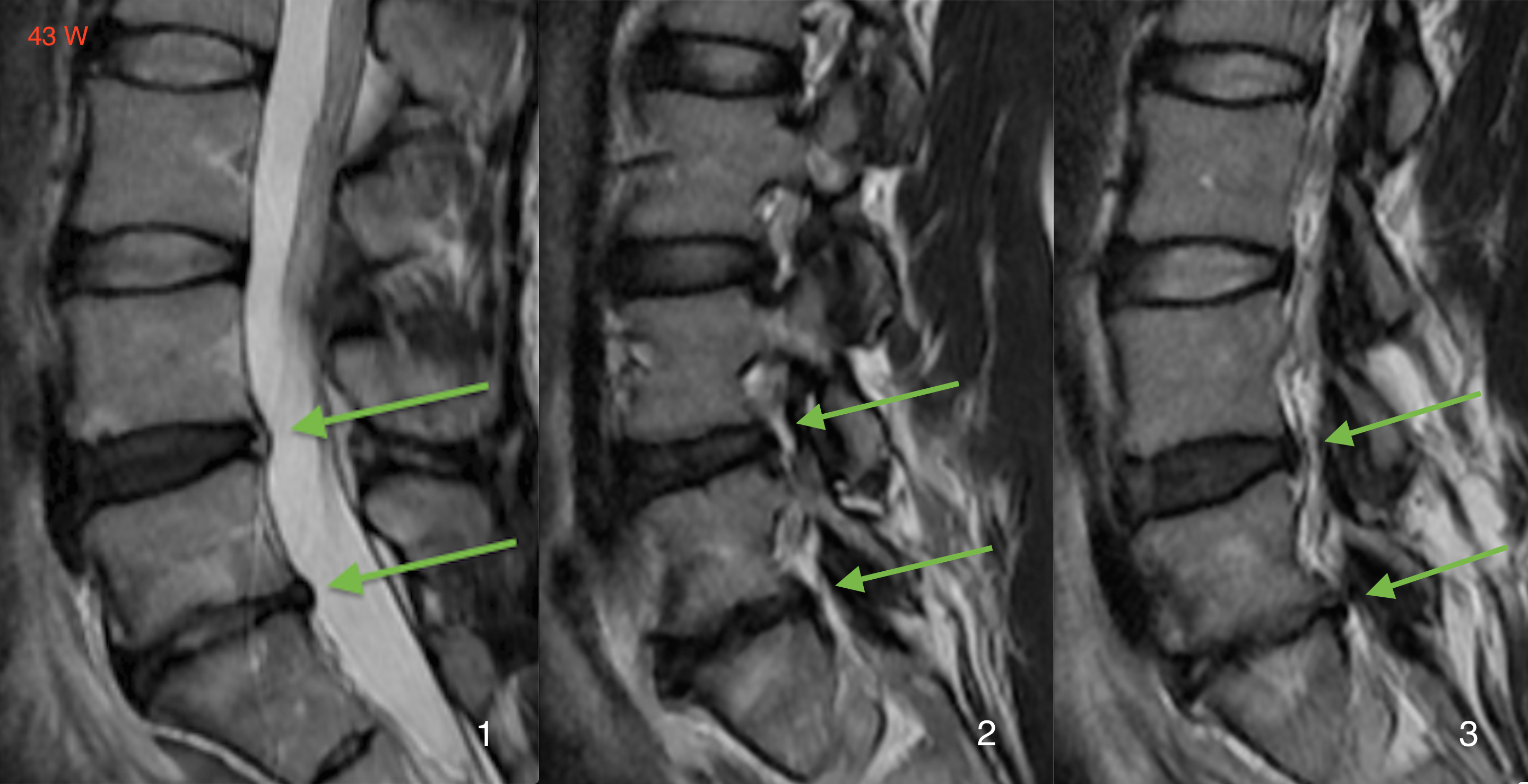
Accurate diagnosis is the foundation of effective treatment. German clinics employ a comprehensive approach. The clinical examination includes assessment of range of motion, neurological status, palpation of paravertebral muscles, and provocative testing. Magnetic resonance imaging (MRI) is the gold standard of diagnostics — it visualizes discs, neural structures and the spinal cord without radiation exposure, allowing precise determination of the degeneration stage and identification of herniations. Computed tomography (CT) provides detailed bone structure assessment, evaluation of osteophytes and stenosis. Functional radiography with flexion and extension views evaluates segment instability. Electromyography (EMG) investigates nerve conduction when nerve root compression is suspected. Laboratory tests exclude inflammatory and systemic diseases.
The examination in German clinics takes 1–2 days. Based on the diagnostic results, a multidisciplinary team — orthopedist, neurologist, spine surgeon — determines the individual treatment strategy.
German physicians adhere to the principle: maximum results with minimum intervention. Preference is given to conservative and regenerative methods. Surgery is applied only when non-surgical treatment is ineffective or in emergency situations.
Pharmacotherapy is used to relieve acute symptoms and as a component of comprehensive treatment. NSAIDs (non-steroidal anti-inflammatory drugs) such as ibuprofen, diclofenac, and celecoxib provide pain and inflammation relief. Muscle relaxants (tizanidine, tolperisone) relieve muscle spasms. Chondroprotectors (glucosamine, chondroitin) offer cartilage protection and partial restoration. B vitamins improve nerve conduction and provide neuroprotection. Epidural blocks — injections of corticosteroids and anesthetics directly to the inflamed nerve root — provide rapid pain relief.
In German clinics, medications are considered a supportive component rather than the primary treatment. The goal is to prepare the patient for active rehabilitation and regenerative procedures.
Physiotherapeutic methods hold a central place in conservative osteochondrosis treatment in Germany. Manual therapy provides spinal segment mobilization and elimination of functional blocks. Therapeutic exercise (individualized programs) strengthens the muscular corset and improves spine flexibility and stability. Shockwave therapy stimulates blood circulation and tissue regeneration. Electrotherapy (TENS, interferential therapy) offers pain relief. Traction therapy decompresses discs through spinal traction. Balneotherapy includes therapeutic baths and aquatic gymnastics. Acupuncture provides reflex action for chronic pain relief.
A fundamentally new solution for treating degenerative spinal diseases is MIBRAR® technology (Minimal Invasive Biologische Regenerative Autologe Rekonstruktion), developed by Prof. Babayan in Munich. Unlike traditional methods aimed at symptom relief, MIBRAR® eliminates the cause of the disease — it triggers regeneration of damaged intervertebral disc tissues.

The essence of the method: First, autologous regenerative concentrate (ARC) is obtained from the patient's venous blood and subcutaneous fat, containing growth factors, mesenchymal stem cells, and anti-inflammatory factors. Then, targeted microperforations are performed in the affected disc area — without incision, only a puncture. Finally, the ARC is transplanted directly into the affected area under ultrasound guidance with 0.1 mm precision (Sono Control Arm™ technology).
Advantages of MIBRAR® for osteochondrosis:
The full list of indications for MIBRAR® therapy is presented on the MIBRAR® indications page.
Surgery for osteochondrosis is indicated when conservative therapy is ineffective for 6–12 weeks or in case of emergency indications (paresis, cauda equina syndrome). German surgeons use modern minimally invasive techniques: microdiscectomy (herniation removal through a minimal 1.5–2 cm incision under an operating microscope), endoscopic discectomy (removal through a 7–8 mm puncture), nucleoplasty (reducing intradiscal pressure in protrusions), spinal stabilization (interbody fusion for pronounced segment instability), and disc replacement (replacing a worn disc with an artificial one while preserving mobility).
After surgery in German clinics, the patient stands on the same day. Discharge occurs within 2–5 days.
The recovery program is selected individually and includes therapeutic gymnastics for strengthening back and abdominal muscles, manual therapy and massage, aquatic gymnastics and balneotherapy, electromyostimulation, and ergonomic training covering proper posture, weight lifting technique, and workstation organization. Rehabilitation takes 4–8 weeks for conservative treatment and 6–12 weeks after surgery. German rehabilitation centers provide a full recovery cycle.
Approximate prices for osteochondrosis treatment in German clinics:
| Service | Price, € | Note |
|---|---|---|
| Comprehensive diagnostics (MRI, examination, tests) | 3,000–5,000 | 1–2 days |
| Conservative treatment (course) | 5,000–8,000 | 7–14 days |
| MIBRAR® therapy | on request | outpatient |
| Microdiscectomy | 10,000–15,000 | 3–5 days inpatient |
| Disc replacement | 20,000–30,000 | 5–7 days inpatient |
All treatment prices in Germany. The final cost is calculated individually after examination.
Germany offers comprehensive diagnostics on state-of-the-art equipment within 1–2 days, innovative MIBRAR® therapy providing tissue regeneration without surgery, a multidisciplinary approach involving orthopedists, neurologists, physiotherapists and rehabilitation specialists, minimally invasive surgery with rapid recovery, a full rehabilitation cycle at world-class clinics, and assistance in your native language at every stage of treatment.
Don't delay your visit to a specialist. The earlier osteochondrosis treatment begins, the higher the chances of full recovery. Leave a request — we will find the optimal clinic and doctor for your case.








 +49 176 17917001
+49 176 17917001 
Or send us a message:



















